The Twilight Zone of the Lucy Letby Case
The prosecution case that was built around Lucy may appear robust but is fragile and at some point will collapse
My heart goes out to the parents of the babies that were the subject of the Lucy Letby trial, whether the thirteen that Lucy was found guilty of harming or the four that she wasn’t. It also goes out to the parents of the babies that are now the subject of the new phase of the Operation Hummingbird investigation, to those of the baby that died in May last year at the paediatric intensive care unit at Birmingham Children’s Hospital where harm is now alleged (I wonder if the ‘poison’ referred to is insulin? I.e. whether it’s one that gets produced naturally by the body), and to all parents of babies that have died on a neonatal unit or experienced some sort of injury in recent years and who may now be worried that harm was inflicted. This is an utterly tragic situation.
As for Lucy, in the wake of the verdicts so much doubt is being cast on her being a killer. People are becoming aware that the main prosecution medical expert Dewi Evans was just a retired paediatrician and thus was not qualified to give evidence, whether about neonatology or about air embolism in neonates.
They are becoming aware that the 1989 paper on which he based his diagnosis was not relevant to the incidents in Lucy’s case.
They are becoming aware that air embolism cannot be diagnosed from an X-ray, let alone whether an air embolism is the result of air having been administered malevolently (it can be the result of sepsis – incidentally, this observation about sepsis was made by one of the prosecution’s very own experts, paediatric radiologist Prof Owen Arthurs).
They are becoming aware that Evans himself said that there was very little research on air embolism, something perhaps the prosecution wished he hadn’t said.
They are becoming aware that Evans may not have been licensed to practice when he got involved in the police investigation. The General Medical Council ‘search the register’ page says that David Richard Evans was ‘Registered without a licence to practise’ from 26 Aug 2015 to 16 Jul 2019 (Evans joined the investigation in May 2017).
They are becoming aware that Evans testified under oath that he was not an expert. According to The Chester Standard, when asked at trial “by Mr Myers if he was being ‘an expert’ in being ‘an expert witness’, Dr Evans replied: ‘I think that’s far too flash for me. My role is to assist the court on some extremely challenging issues. I call myself an independent medical witness, not an expert.'”
However, his LinkedIn profile says that he provides “expert medical advice regarding clinical issues where child abuse is suspected or where there are allegations of clinical negligence”. (Also, Dr Evans, shouldn’t you have been investigating whether there had abuse or negligence, not where ‘it is suspected’, thus eliminating the potential for confirmation bias? No mention of you being a retired consultant paediatrician either which some might argue is misleading.)
They are becoming aware that Evans is registered on the site Expert Witness, the site that says “Let us do the hunting whatever expert you need. Please call our free SearchLine today on 0161 834 0017” though his entry now lists only his name and nothing else.
They are becoming aware that Evans probably got paid for his services, and by the prosecution, an obvious conflict of interest.
They are becoming aware that it was not Evans who was approached by the police but the other way round. He approached the National Crime Agency in May 2017 by email. The below is an extract from The Chester Standard published on 7 March 2023 titled, ‘Medic denies ‘touting for job’ helping Lucy Letby police probe’.
In his message to “Nick” at the NCA’s national injuries database, Dr Evans wrote: “Incidentally I’ve read about the high rate of babies in Chester and that the police are investigating. Do they have a paediatric/neonatal contact? I was involved in neonatal medicine for 30 years including leading the intensive care set-up in Swansea. I’ve also prepared numerous neonatal cases where clinical negligence was alleged. If the Chester police had no-one in mind I’d be interested to help. Sounds like my kind of case. I understand that the Royal College (of Paediatrics and Child Health) has been involved but from my experience the police are far better at investigating this sort of problem.”
(Incidentally, Dr Evans, where did you ‘read about the high rate of babies in Chester and that the police are investigating’? It wasn’t public knowledge at that time. Might someone have told you about it rather than you having read about it?)
They are becoming aware that he was admonished by a judge in a previous case for presenting worthless evidence.
When asked about the judge’s admonishment in that previous case, Evans replied “This is a one-off for me”. Hmm, not sure about that, Dr Evans.
Evans had been involved in controversial cases on several previous occasions. Here are some of them.
#1: The case of a 2-year-old girl and her 4-year-old elder brother
Extracts from the judgement:
“In his judgment the trial judge was critical of Dr Evans, suggesting that his evidence should have been more considered and structured than in fact it was.”
“The fact that the trial judge in the present case was unimpressed by Dr Evans left him open to being more persuaded by the evidence of Dr Primrose.”
“They also agreed that there were probably two separate impacts or events causing the injuries rather than one, a departure from Dr Evans’ written report.”
#2: The case of a six-week-old baby who died in 2018
Extract from the article:
“Winchester Crown heard from consultant paediatrician Dr Dewi Evans who also said the baby, who died on February 11, suffered an “intentional” bite to the nose.”
“Dr Evans told the jury he thought the defendants’ accounts of either the baby being dropped or falling from a sofa didn’t explain the injuries, which included a fractured femur, rib fractures, and the bite to the nose.”
#3: The case of abuse of a young girl by the Neath Port Talbot State Child Protection Machinery
Extract from the article:
“Behind the scenes Dr Dewi Evans of Singleton Hospital had already been manipulating events. Writing to Dr Dazell of Alder Hey Liverpool on 9 April 1997, he provides a summary of Bonnie’s case, which contains errors and untrue statements. In particular he describes the operation to remove Bonnie’s appendix as revealing an appendix that was “long and swollen”. He also describes the recovery as uneventful apart from some “redness around the appendectomy scar”. Either Evans was misinformed or this was a blatant lie, since Bonnie’s appendix was normal, and she had suffered a massive post operative infection and abscess of the wound.”
#4: The case of a 17-month old baby girl who was admitted to the Erne Hospital in Enniskillen in 2000 and who later died
According to the article, “Dr Dewi Evans, a consultant paediatrician from the Department of Child Health in Swansea, criticised the hospital at an inquest today dealing with the death of Lucy Rebecca Crawford.”
#5: The case the collapse and subsequent death in 2017 of a five-month-old girl
Philip Peace, 42, of Himley Road in Dudley, denied murder and manslaughter of his daughter, Summer.
According to the article, “[Dr Evans] said the collapse would not have been caused by pneumonia and concluded, in his opinion, that it was caused by head trauma, a judge heard.
The article went on the say that:
“Mr Michael Turner QC, defending Summer’s father Philip Peace in the trial, questioned Dr Evans to see if it was possible the condition could be pre-existing. Mr Turner cited sounds heard by paramedics, described as noisy and bubbling, when they listened to Summer’s chest as possibly being evidence of the condition. Dr Evans, in response to the cross-examination, said it could be explained through transmitted noises – noises from the throat – due to the baby’s size. He added it could also be – in conjunction with the first explanation – could be food or liquid being aspirated into her lungs which causes aspiration pneumonia.”
#6: The case of Claire Roberts who died at the Royal Victoria Hospital for sick children in October 1996.
The note for Professor Brian Harding in the case cites “The clear difference of opinion between the pathologists concerned, with Dr. Dewi Evan’s hypothesis perhaps providing evidence in favour of Dr Herron’s analysis rather than that of Dr Harding.”
Other exhibits in the case relating to Evans can be found here, here, and here.
Then there is the excellent Law, Health and Technology Newsletter and its article LL Part 6: The Incredible Dr Dewi Evans. I shall let you read it.
In another killer caregiver case, Dutch nurse Lucia de Berk was sentenced to life imprisonment in 2003 for four murders and three attempted murders of patients under her care. In 2004, after an appeal, she was convicted of seven murders and three attempted murders. According to statistician Richard Gill, who campaigned for her innocence, Lucia was eventually exonerated because the original expert toxicologist withdrew his testimony. He did this because another toxicologist (who had been suggested to the Court by the defence and whom the Court accepted) came along with the correct interpretation of the toxicology data. And he saved face when he withdrew his testimony because he was able to blame the the public prosecutor and the Court for withholding critical information from him.
In Lucy’s case, the Rex v Lucy Letby website sets out systematically what it believes to be the correct science in relation to air embolism, all carefully referenced. Moreover, there are likely to be those with even greater specialist expertise coming forward to rebut what Evans presented at trial. (Incidentally, the Rex v Lucy Letby website also sets out different and carefully researched scientific interpretations in relation to insulin , air in the gut and sudden collapse, so experts may well come forward in due course offering different opinions on those too).
Dr Evans, you have the chance to withdraw your evidence now. Don’t wait until you are forced to. Please. A young woman sits in prison on a full life term. It’s possible you weren’t given everything by the prosecution, that you were a victim too. People would be sympathetic.
The public is also becoming aware that the maternity unit of The Countess of Chester where Lucy worked was in chaos, and was still in chaos in 2022, five years after Lucy was taken off the ward.
They are becoming aware that there were numerous incidents on the unit that Lucy was not charged with. And, most importantly, they are becoming aware that the death rate on the unit did not fall after Lucy was taken off it. In fact, it rose.
In relation to this last point, I first raised suspicion about Lucy’s case over ten months ago when her trial started. In my blogs about Lucy’s case that I published in June and July this year I cited Countess of Chester Hospital data obtained through a freedom of information request that showed there had been a spike in neonatal deaths in 2015 and 2016. I derived from this data that there had also been a spike in deaths that Lucy had not been charged with, and that therefore the prosecution was essentially asking the jurors to believe that as well as a serial killer on the unit there was something else causing the deaths (in fact, I don’t believe the jurors did see this data).
I then saw the Rex v Lucy Letby website which presented ONS data showing that neonatal deaths in Chester and Cheshire West had actually risen after Lucy was taken off the unit, that there had been no sharp fall per the hospital data. How could this be?
Some have rightly pointed out that the ONS data is for the Chester and Cheshire West while the FOI request data is for The Countess of Chester only. Well, we have everything we need to calculate the neonatal death rate (deaths per 1,000 births) for Chester and Cheshire West not including The Countess of Chester.
The result is as below:
Table 1: Deaths per 1,000 births for Chester and Cheshire West not including The Countess of Chester (rate for England also included for comparison)

Rate 1 is calculated based on the inclusion of two deaths in August and October 2015 that Lucy was charged with that were not in the FOI data (since these increased the rate at CoCH, they lowered the rate outside CoCH). Rate 2 is based on FOI data that do not include these two deaths.
Now, a negative death rate is absurd, so there must be something wrong with one or both data sources. Also, if the neonatal death rate in Chester/Cheshire West outside of CoCH in 2018 was 7.2 per 1,000 deaths, someone should have raised the alarm, given that the rate for the whole of England that year was 2.6. Nobody did.
As for the media coverage since the verdicts were announced on 18 August, it too is getting absurd. Below are some examples.
Fact: It is unusual for a serial killer to use different methods.
Media response: Ah ha! A sign of her deviousness.
Fact: The unit was in chaos.
Media response: Ah ha! Lucy must have taken advantage of that to hide her killing spree. (C’mon, peeps, which is more likely?)
Fact: Lucy was calm during police interviews.
Media response: Ah ha! How cold! How calculating!
In relation to the famous Post It note which many claim is a confession, according to the BBC’s Lucy Letby: The Nurse Who Killed, the police discovered it “inside her diary”. Why did Lucy not write in her diary? Seems like the obvious place to write those sort of innermost thoughts. And why did the police feel the need to move the note to take a photograph of it rather than leaving it where it was found? (see Figure 1.)
Might Lucy have written it somewhere else? That might explain why it was not written in her diary but on a Post It note, along with many other scribblings crammed on the little square piece of paper (at home she surely had plenty of paper so no need for crammed writing. And she had a diary). Finding the note at home was certainly supportive of the police’s case. She was in her safe space, after all. As opposed to, for example, writing it in her prison cell after a police interview during which she had been put under extreme pressure. For example.
Figure 1: Police photo of the famous Post It note
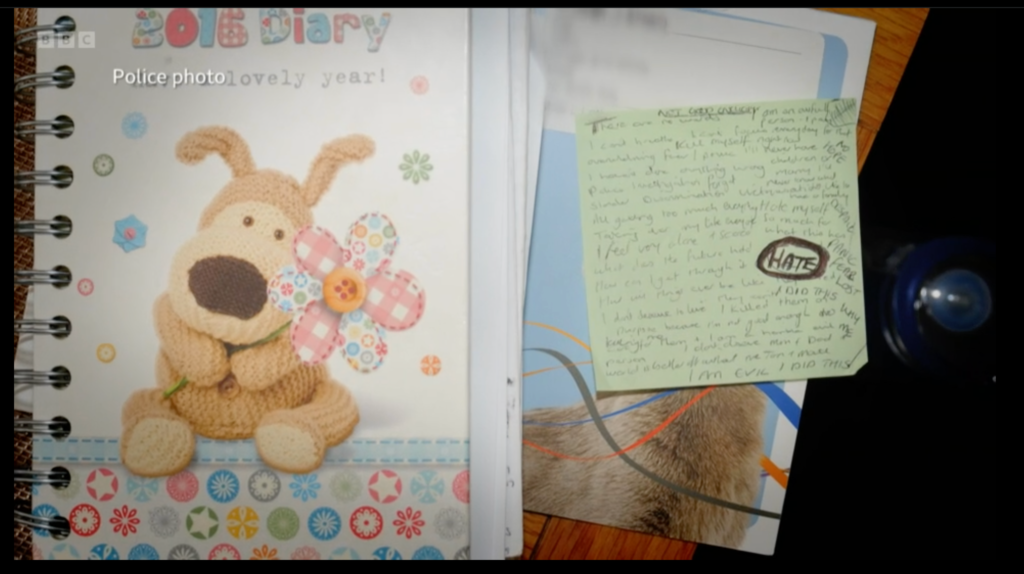
Source: BBC Panorama (Lucy Letby: The Nurse Who Killed)
Fact: She wrote “I am evil, I did this” and “I killed them” on a note.
Media response: A ha! A confession!
Well, no. At around 45:50 on the BBC’s Lucy Letby: The Nurse Who Killed, renowned criminologist David Wilson says in relation to the note:
Well, it seems like a confession. But it might be she is saying, ‘It is alleged I killed them. It is alleged I am evil, I did this’. I have worked on a number of murder cases whereby you get people writing strange notes all the time. It’s evidence of their underlying stress, mental health problems. It’s not necessarily evidence of guilt. I just think this is the ramblings of someone who is under extreme psychological pressure.
Had Lucy been a killer, it is very likely she would have confessed. That she is likely innocent, it is extraordinary that she did not. More pertinently, any confession would have been a false one. False confessions are real phenomena. They happen. Many exonerations are based on it being determined that the convicted person made a false conviction. Under incessant questioning by police, people start to believe they did it. They want the questioning to stop. They are told that confessing will help them.
It also seems absurd to me that in virtually the same week that wrongly-convicted (on the back of flawed DNA evidence) Andrew Malkinson had his case overturned after spending 17 years in prison, few wondered if Lucy’s conviction might just possibly have been the result of similarly bad evidence. Quite the opposite.
Immediately after Lucy’s verdict, the neonatal consultants at CoCH were on TV blaming the hospital for failing to heed their warnings about Letby. Why, if they suspected Lucy of harming babies, did they not tell the police? Or the coroner? Or do everything in their powers to get Lucy off the unit? Surely, as consultants they had the power to do this. More to the point, they had an ethical obligation. They may well also have had a legal obligation.
While Lucy is at the centre of this case, fighting what could well be an unsafe conviction is not ultimately about her. No. It is about protecting all NHS healthcare workers in future from unfounded accusations and possible wrongful convictions. It is about protecting everyone from becoming a victim of poor scientific evidence presented in the courtroom. It is about you (and if you think this couldn’t happen to you, think again).
There is a huge disconnect between on the one hand the stark reality of the verdicts and the public’s strong belief that Lucy is Britain’s worst baby killer, and, on the other, the reality of the evidence supporting the case for there having been a miscarriage of justice. It is like being in The Twilight Zone.
Lucy must be Britain’s worst baby killer. After all, she failed to murder six babies on seven occasions. Who’d have thought it was so hard to kill a tiny, vulnerable, premature baby.
© Chimp Investor Ltd